The Tamil Nadu Assistant Surgeon (General) Recruitment 2025 highlights India’s medical employment crisis, where 25,172 doctors competed for only 1100 government posts. With a 23:1 ratio, category wise seat fragmentation, repeated exams, and take home pay near ₹85,000, the notification exposes severe doctor overproduction and lack of workforce planning.
The Tamil Nadu Medical Services Recruitment Board notification for Assistant Surgeon General recruitment in 2025 should alarm every medical student, intern, resident, and policymaker in the country. A total of 25,172 doctors appeared for an exam offering just 1100 posts. That is a competition ratio of approximately 23 doctors for every single government seat. This is not an employment drive. This is a mirror held up to a collapsing workforce planning system.
The Illusion of Opportunity Created by a Big Number
To a non medical observer, 1100 posts may sound generous. In reality, it is painfully inadequate. Tamil Nadu alone produces several thousand MBBS graduates every year from government and private colleges. Add FMGs who have cleared licensing exams, add repeat candidates from previous recruitment cycles, and suddenly 1100 seats look like crumbs scattered among a starving crowd. The system keeps advertising small batches of jobs and calling it progress.
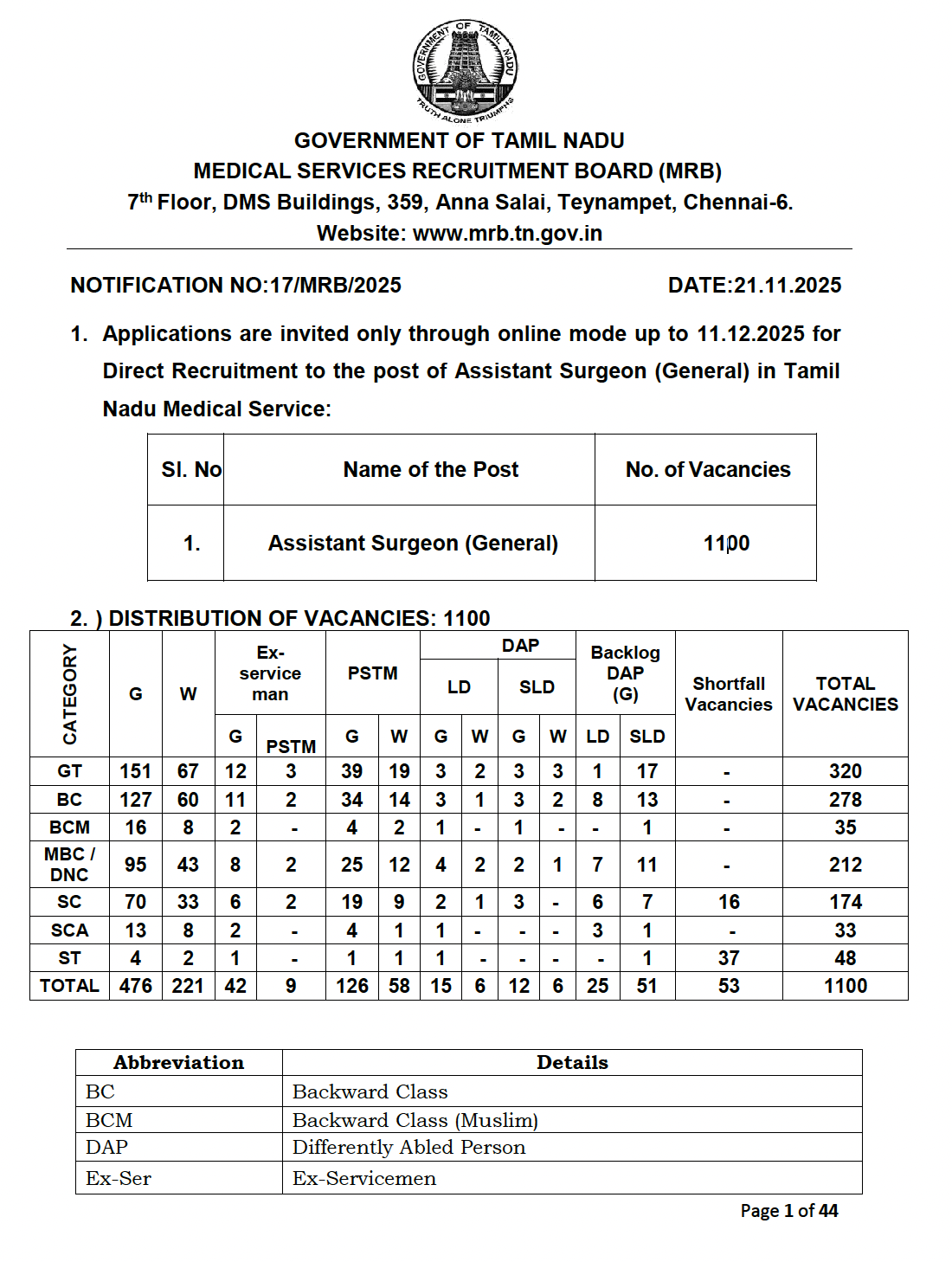
Category Wise Distribution Further Fragments the Seats
The 1100 posts are divided across GT, BC, BCM, MBC or DNC, SC, SCA and ST categories, along with horizontal reservations for women, ex servicemen, persons studied in Tamil medium and differently abled candidates. Once this distribution is applied, the actual number of seats available to a candidate within their category becomes extremely small. In some categories, candidates are effectively competing for single digit numbers of posts. The conversation about merit conveniently ignores how narrow the funnel really is.
25,172 Applicants: The Number That Should Have Triggered Panic
More than twenty five thousand doctors registering for one state level recruitment exam is not a healthy sign. It reflects desperation. Many of these candidates are already working as temporary medical officers, tutors, contractual doctors or private hospital employees with poor job security. Government service remains one of the few avenues offering stability, fixed hours and some protection from exploitation. When that avenue opens for only 1100 people, the rest are left stranded.
Overproduction of Doctors Without Absorption Capacity
Medical colleges have been expanding rapidly over the last decade. Seats are increased every year, new colleges are approved, and the narrative sold is that India needs more doctors. What is rarely discussed is where these doctors are supposed to work. Government job creation has not kept pace. Primary health centres, government hospitals and public health systems have vacancies on paper, but sanctioned posts remain limited. The result is a surplus workforce with no structured absorption plan.
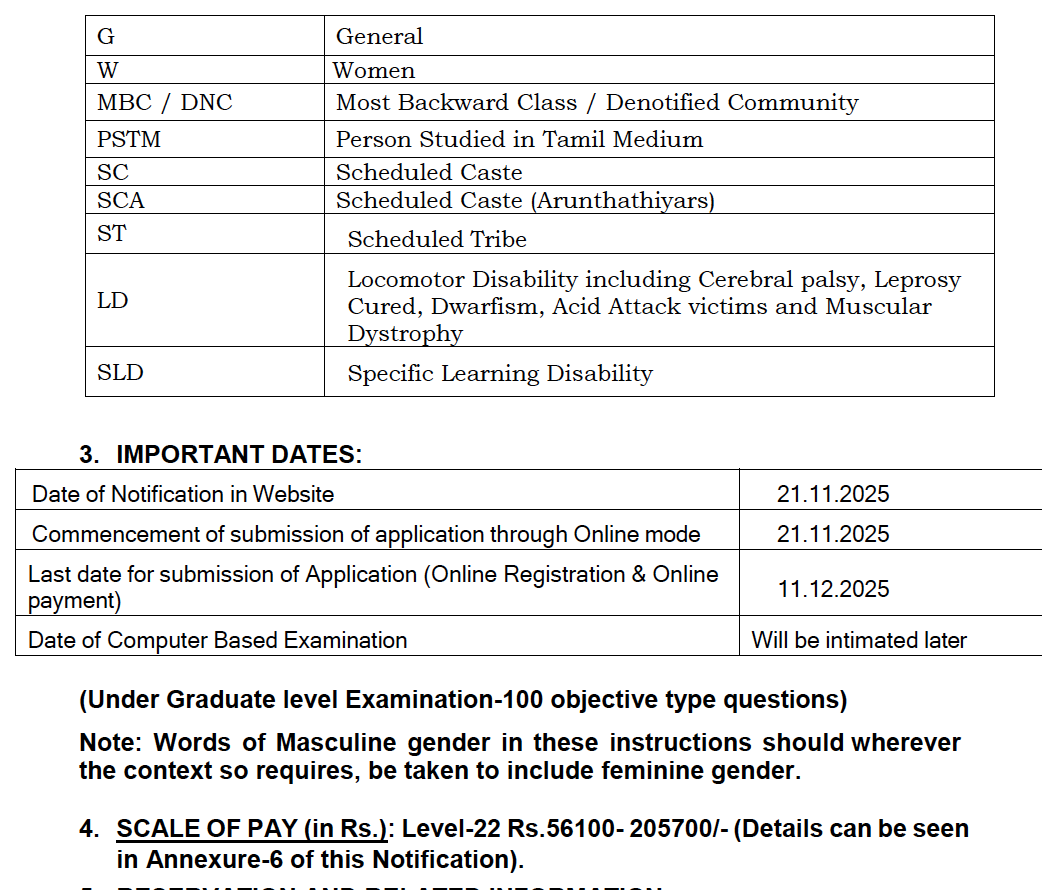
The Assistant Surgeon Salary Myth
The advertised pay scale for Assistant Surgeon is Level 22, ranging from ₹56,100 to ₹2,05,700. This figure is often used to project government jobs as highly lucrative. The ground reality is different. After deductions, the monthly take home salary is around ₹80,000 to ₹85,000. This comes after NEET UG, five and a half years of MBBS, internship, compulsory service and now another competitive exam. For many doctors in their late twenties or early thirties, this salary barely compensates for the years of delayed financial independence.
Another Exam After a Decade of Exams
Selection is through a computer based examination consisting of 100 undergraduate level objective questions. Doctors who have already survived NEET UG, internal assessments, final MBBS exams, internship evaluations and licensing hurdles are once again reduced to MCQ solving machines. Exams have become the default tool to manage excess supply rather than addressing structural issues like job creation and workforce distribution.
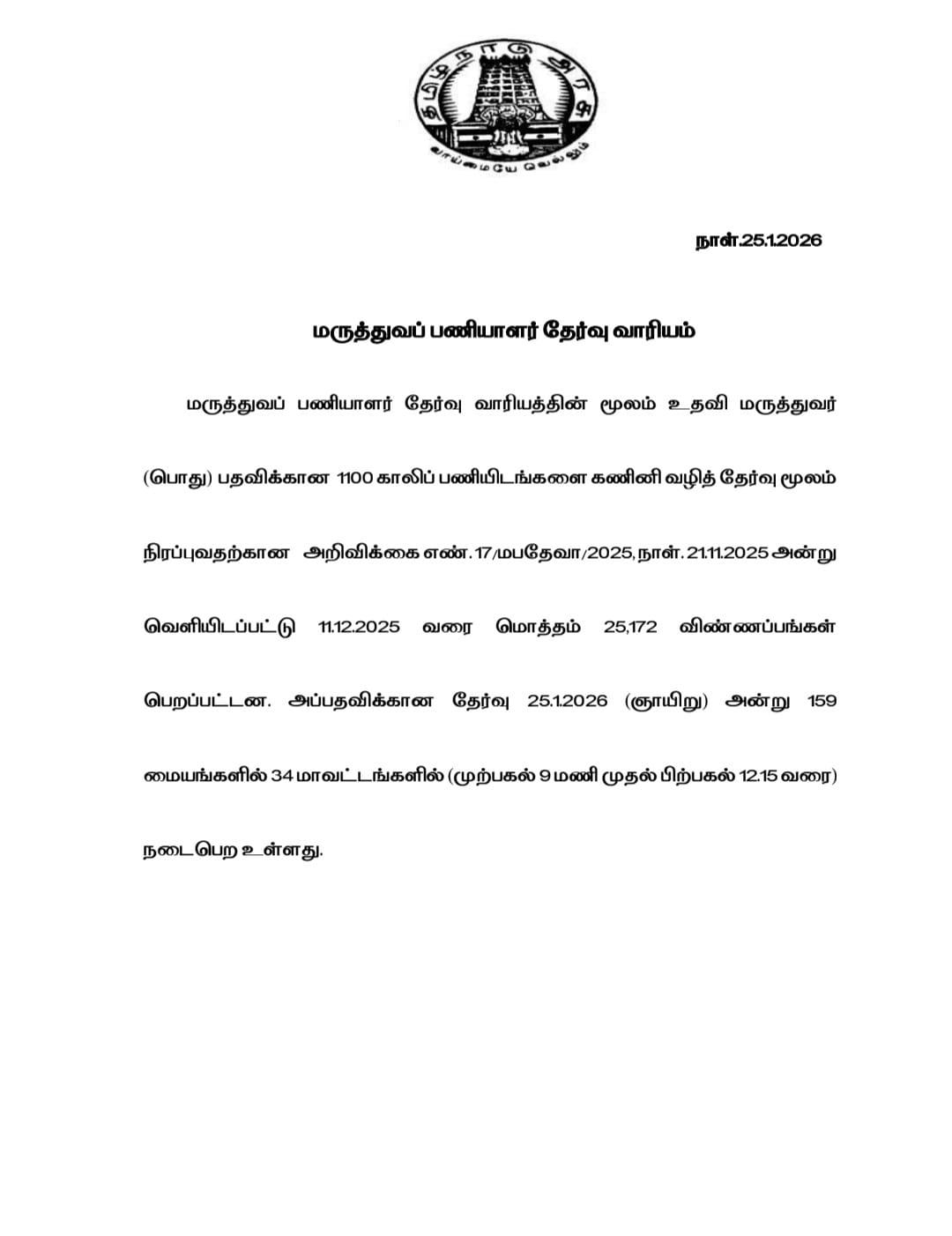
Exam Conduction Shows the Scale of the Crisis
Applications opened on 21 November 2025 and closed on 11 December 2025. 25,172 candidates applied. The examination was conducted on 25 January 2026 across 34 districts of Tamil Nadu. This scale of participation for such a limited number of posts is not competitiveness. It is crowding caused by lack of alternatives. Most candidates walked into the exam hall knowing that statistically, failure was more likely than success.
What Happens to the Remaining 24,000 Doctors
Once results are declared, 1100 candidates move ahead. The remaining 24,000 plus doctors do not disappear. They continue working in insecure contractual roles, prepare again for the next exam, attempt PG entrance, migrate abroad, or leave clinical medicine altogether. Burnout, frustration and resentment are not individual failures. They are predictable outcomes of a system that produces more doctors than it can employ.
The Uncomfortable Questions No One in Power Answers
If the state genuinely requires more doctors, why are sanctioned posts so limited? If there is no requirement, why is medical education expanding every year? Who benefits from this imbalance? Medical education has increasingly become a revenue driven sector, while employment planning remains stagnant. Doctors are trained without a career roadmap and then blamed for unemployment or migration.
Government Jobs Have Become Survival Prizes
A government medical post is no longer just a career choice. It has become a survival prize in an oversaturated market. Stability, predictable hours and some degree of dignity are now luxuries that only a small fraction of doctors can access. The rest are expected to adjust, struggle quietly or accept exploitation as part of the profession.
Conclusion: A Recruitment Notification That Exposes a Broken System
This recruitment drive should not be celebrated as progress. 25,172 doctors competing for 1100 posts at a ratio of 23:1 is evidence of policy failure, not meritocracy. Until medical education expansion is matched with workforce planning, job creation and realistic career pathways, such notifications will continue to expose the same truth. India is not facing a shortage of doctors. It is facing a crisis of planning.
The National Testing Agency has officially announced the new date for the NEET UG 2026 re examination after cancelling the earlier exam due to the alleged paper leak controversy. The re exam will now be conducted on June 21, 2026, affecting more than 22 lakh medical aspirants across India.
PMOS, previously known as PCOS, is a newly renamed condition that better reflects its hormonal and metabolic effects beyond the ovaries. The change from Polycystic Ovary Syndrome to Polyendocrine Metabolic Ovarian Syndrome highlights its association with insulin resistance, obesity, fertility issues, and long term health risks affecting millions of women worldwide.
A doctor in Bhilwara allegedly attempted suicide by consuming phenyl after accusing a private hospital operator of financial exploitation, unpaid salary, mental harassment, and police inaction. The incident has sparked concern over workplace conditions and disputes in the medical profession.