What Actually Happened?
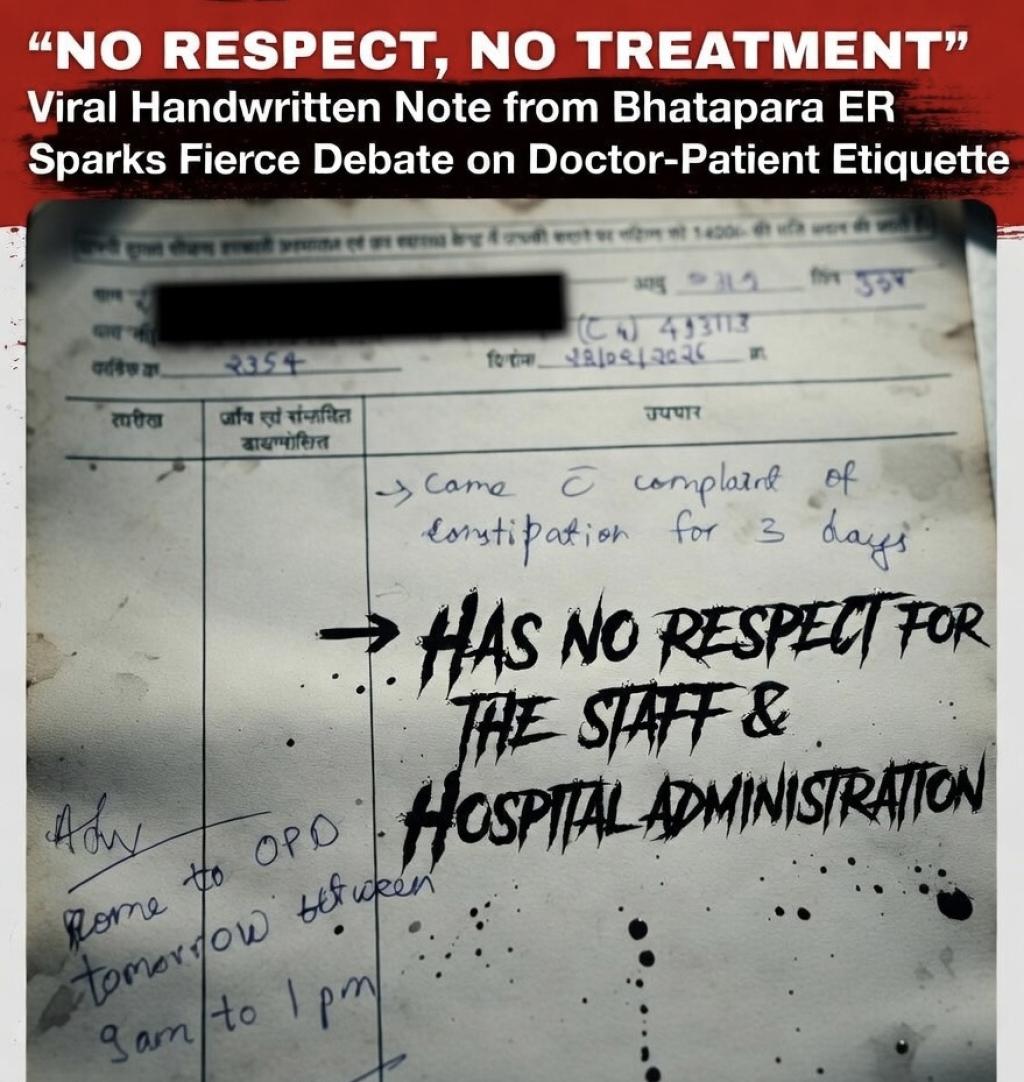
From the circulated image:
•The patient presented to the Emergency Room (casualty) with constipation for three days.
•No severe red-flag symptoms (e.g., intense abdominal pain, vomiting, blood in stool, or distension suggesting obstruction) were mentioned.
•The doctor noted alleged disrespect and misbehavior.
•Instead of providing symptomatic relief (like a laxative prescription or basic advice), the doctor refused to proceed in the ER and asked the patient to return the next day during outpatient hours (roughly 9 AM to 1 PM).
This is not outright “denial of emergency care” in the life-threatening sense constipation is rarely an emergency unless complicated but it highlights triage decisions in overburdened public facilities.
Why Doctors Might Feel Justified
Government hospitals in India, especially in smaller towns like Bhatapara (about 100 km from Raipur), handle massive patient loads with limited staff. Emergency Rooms are meant for true emergencies: trauma, heart attacks, strokes, acute abdomen, etc. Simple constipation often due to diet, dehydration, or lifestyle is typically managed in OPD with over the counter advice or mild laxatives.
Many doctors argue:
•Misuse of emergency services:Patients (or attendants) often crowd casualty for non-urgent issues, delaying care for critical cases.
•Verbal and physical abuse:Assaults on doctors are alarmingly common in India. The note’s emphasis on “no respect for staff and doctors” reflects frustration from repeated rudeness, demands, or threats when expectations aren’t met instantly.
•Self-preservation:In a high-stress environment, refusing non-emergent care to disruptive individuals protects mental health and safety.
Supporters on social media, especially in medico groups, see this as a rare pushback: “Respect is reciprocal. Abuse shouldn’t be rewarded with free service.”
The Counterarguments: Ethics and Duty
Medical ethics, as per Indian Medical Council/NMC guidelines, emphasize that doctors in public hospitals have a duty to treat patients without discrimination. Refusing care based on behavior can cross into unprofessional territory, especially if it delays basic symptomatic relief.
Critics point out:
•Constipation isn’t trivial for everyone:In elderly patients, those with comorbidities, or in cases of underlying obstruction, it can worsen quickly.
•Power imbalance:Patients in government setups are often poor, illiterate, or desperate. Writing accusatory notes instead of de-escalating or involving security feels punitive.
•Documentation issues:The note focuses more on blame than clinical reasoning (e.g., “no red flags, non-emergent”). Better documentation could defend the decision legally and ethically.
•Systemic failure:Overcrowding, understaffing, and poor security fuel these conflicts. Blaming the patient ignores root causes.
Even some doctors acknowledge: “The intent might be right, but the execution public shaming via note was not professional.”
Broader Implications for Indian Healthcare
This is not an isolated incident. Similar stories surface regularly doctors being assaulted over delays and patients being denied non-emergent care amid chaos. It underscores:
•The need for better triage systems in casualty departments.
•Mandatory security and de-escalation training.
•Public awareness campaigns on when to use ER vs. OPD.
•Stronger protections for healthcare workers under laws like the Epidemic Diseases Amendment Act or state-specific ordinances.
Ultimately, respect must flow both ways. Patients deserve dignified, timely care; doctors deserve safety and courtesy. In an ideal world, a quick examination and basic laxative advice could have resolved this without escalation. However, in reality, strained resources and frayed tempers turn minor issues into viral controversies.
What do you think? Was the doctor right to draw a line, or should the ER always provide at least basic relief regardless? The debate continues, but one thing is clear empathy and mutual respect are essential to improving the doctor-patient relationship.